Sleep Apnea for Kids
Children’s Obstructive Sleep Apnea (OSA)
 Does your child snore? Does your child show other signs of disturbed sleep: long pauses in breathing, much tossing and turning in the bed, chronic mouth breathing during sleep, night sweats (owing to increased effort to breathe)? All these, and especially the snoring, are possible signs of obstructive sleep apnea (OSA), which is more common among children than is generally recognized. It’s estimated than 1 to 4 percent of children suffer from obstructive sleep apnea, many of them being between 2 and 8 years old.
Does your child snore? Does your child show other signs of disturbed sleep: long pauses in breathing, much tossing and turning in the bed, chronic mouth breathing during sleep, night sweats (owing to increased effort to breathe)? All these, and especially the snoring, are possible signs of obstructive sleep apnea (OSA), which is more common among children than is generally recognized. It’s estimated than 1 to 4 percent of children suffer from obstructive sleep apnea, many of them being between 2 and 8 years old.
Common Warning Signs of Obstructive Sleep Apnea (OSA):
- Snoring during Sleep
- Appearing to have difficulty breathing during sleep
- Experiencing night terrors, sleep walking, or bed wetting
- Mouth breathing
- Daytime hyperactivity or being irritable, agitated, aggressive, and cranky
- Having problems in school
- Difficulty in waking up in the morning
- Appearing very sleepy or actually falling asleep during the day
OSA symptoms in children vary depending on their age. If a child is younger than five years old symptoms include snoring, sleeping with an open mouth, sweating, daytime restlessness and waking up during the night. A child five years and older will also have the same symptoms but also will experience behavior problems, a short attention span, have a hard time with school work and even might wet the bed.
As with adults, children with OSA almost always snore. The one key difference between an adult and a child, the child with sleep apnea won't grow as quickly and they don't fall asleep during the day (no matter how hard you try). This developmental delay can cause the right side of their heart to get bigger. Therefore, if you feel your child has OSA or developing sleep apnea, he should be tested right away.
Studies have suggested that as many as 25 percent of children diagnosed with attention-deficit hyperactivity disorder may actually have symptoms of obstructive sleep apnea and that much of their learning difficulty and behavior problems can be the consequence of chronic fragmented sleep. Bed-wetting, sleep-walking, retarded growth, other hormonal and metabolic problems, even failure to thrive can be related to sleep apnea.
Making the Diagnosis
 As in adults, polysomnography is the only tool for definitive diagnosis and assessment of the severity of pediatric obstructive sleep apnea. It needs to be conducted during an overnight stay in a sleep lab, with the test conducted by technologists experienced in working with children and the data interpreted by a sleep medicine physician with pediatric experience. At present there is too little data as to the feasibility and validity of pediatric home studies to list them as a reliable alternative.
As in adults, polysomnography is the only tool for definitive diagnosis and assessment of the severity of pediatric obstructive sleep apnea. It needs to be conducted during an overnight stay in a sleep lab, with the test conducted by technologists experienced in working with children and the data interpreted by a sleep medicine physician with pediatric experience. At present there is too little data as to the feasibility and validity of pediatric home studies to list them as a reliable alternative.
Other reasons your child may have sleep apnea is due to being overweight. Excess weight on the neck applies pressure to the airway. Weight management, including nutritional, exercise, and behavioral elements, should be strongly encouraged for all children with OSA who are overweight or obese. An adequate nightly duration of sleep is an important component of weight management.
Allergies may trigger OSA and can be treated with nasal steroids which may improve the nasal obstruction.
Treatment
 Surgical removal of the adenoids and tonsils is the most common treatment for pediatric OSA. In uncomplicated cases, the operation results in complete elimination of OSA symptoms in 70 to 90 percent of the time. Owing to post-operative swelling, full resolution of the OSA symptoms may not occur for six to eight weeks.
Surgical removal of the adenoids and tonsils is the most common treatment for pediatric OSA. In uncomplicated cases, the operation results in complete elimination of OSA symptoms in 70 to 90 percent of the time. Owing to post-operative swelling, full resolution of the OSA symptoms may not occur for six to eight weeks.
Airway Focused Orthodontics
We are strong proponent of early interventional orthodontic care to increase the breathing capacity in children. Oral appliances can be used with great success in children as young as the age of 6. Expansion of both upper and lower jaws is possible in children ( between the ages of 7-9) as their facial bone growth has not yet been fully developed.
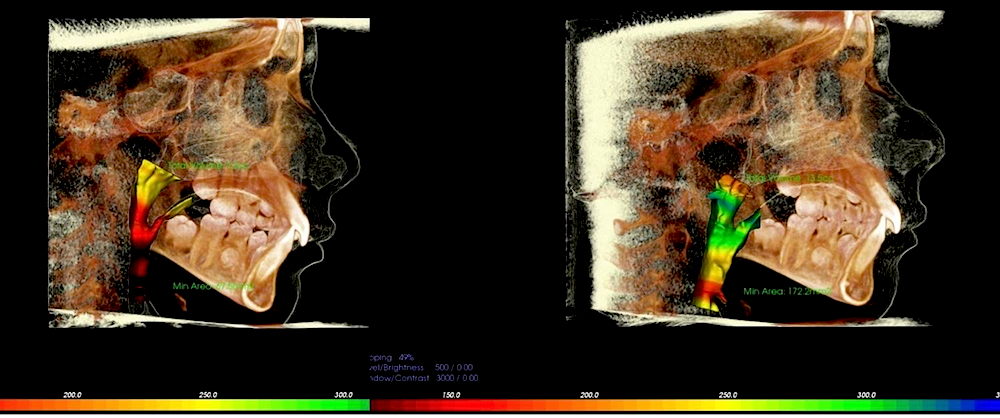
This is a comparison of 3-D images evaluating the internal airway dimensions of a patient suffering from obstructive sleep apnea. Early orthodontic treatment using oral appliances only (no surgery) resulted in a greater than 3x increase in airway capacity!!!
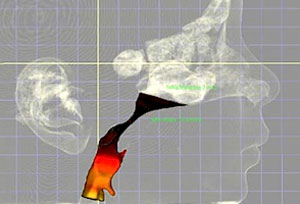
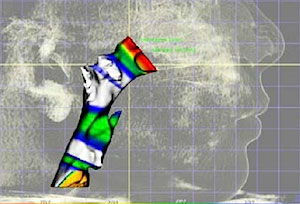
Another impressive comparison of 3-D modelling of the airway. Image on Left shows narrow airways before treatment. Image on the Right shows airway enlarged 3-4x original size after orthodontic care. Sleep apnea symptoms fully resolved after orthodontic treatment. Truly AMAZING results.

J.B. Phase 1: Early Expansion + Limited Braces 12 months Obstructive Sleep Apnea
Here is another great example of early orthodontic treatment for growth modification (phase 1) at Erik Swanson Orthodontics. This patient suffered from obstructive sleep apnea with a reduced ability to be able to breathe properly. Mom noticed her son did not sleep well, was irritable, and his grades were suffering at school. He was referred to us by his dentist because his top teeth on one side were abnormal in that they were actually inside his lower teeth (posterior crossbite). The great news for the family is that we specialize in Airway Focused orthodontics and early interventional orthodontic care. We proposed a game plan that would address both his airway needs as well as dental. He successfully completed his care in 12 months. Mom reports that he no longer snores, happier overall, and his grades have improved as well! AMAZING RESULTS !!! These gentle skeletal corrections are only possible during the early ages 7-9.